Hydrocephalus as the missing variable in tuberculous meningitis trials
Infectious Diseases and Tropical Medicine 2026;
12
: e1865
DOI: 10.32113/idtm_202607_1865
Topic: Tuberculosis
Category: Editorial
Tuberculous meningitis (TBM) remains the most lethal form of tuberculosis, with mortality rates that have changed little despite advances in antimicrobial therapy and adjunctive immunomodulation. Over the past two decades, multiple randomized controlled trials have evaluated intensified antitubercular regimens and adjunctive corticosteroid strategies, yet most have failed to demonstrate substantial improvements in survival1-3. These findings are often interpreted as evidence of limited therapeutic efficacy. However, such a conclusion may be incomplete, as important determinants of outcome may not be adequately captured in current trial designs.
Most TBM trials are built on the premise that mortality is primarily driven by uncontrolled infection or dysregulated inflammation. While both are undoubtedly important, this framework may underappreciate the role of intracranial pathophysiology, particularly hydrocephalus and its downstream effects on intracranial pressure (ICP)4-6. Hydrocephalus is common at presentation, frequently evolves during the disease course, and is strongly associated with poor outcomes. It may represent both a marker of disease severity and a potentially modifiable contributor to secondary brain injury, although the relative contribution of these roles remains uncertain.
Raised ICP can lead to reduced cerebral perfusion, brainstem compression, and irreversible neurological injury within a timeframe that may precede the therapeutic effects of antimicrobial or anti-inflammatory interventions. Consequently, it is plausible that some patients may experience adverse outcomes related to intracranial hypertension despite receiving antimicrobial and anti-inflammatory therapies. In such circumstances, the benefits of pharmacological interventions may be underestimated because patients experience early ICP-mediated injury before those therapies can exert their intended effects (Figure 1).
Figure 1. Proposed causal framework linking infection, inflammation, hydrocephalus, and clinical trial outcomes in tuberculous meningitis.
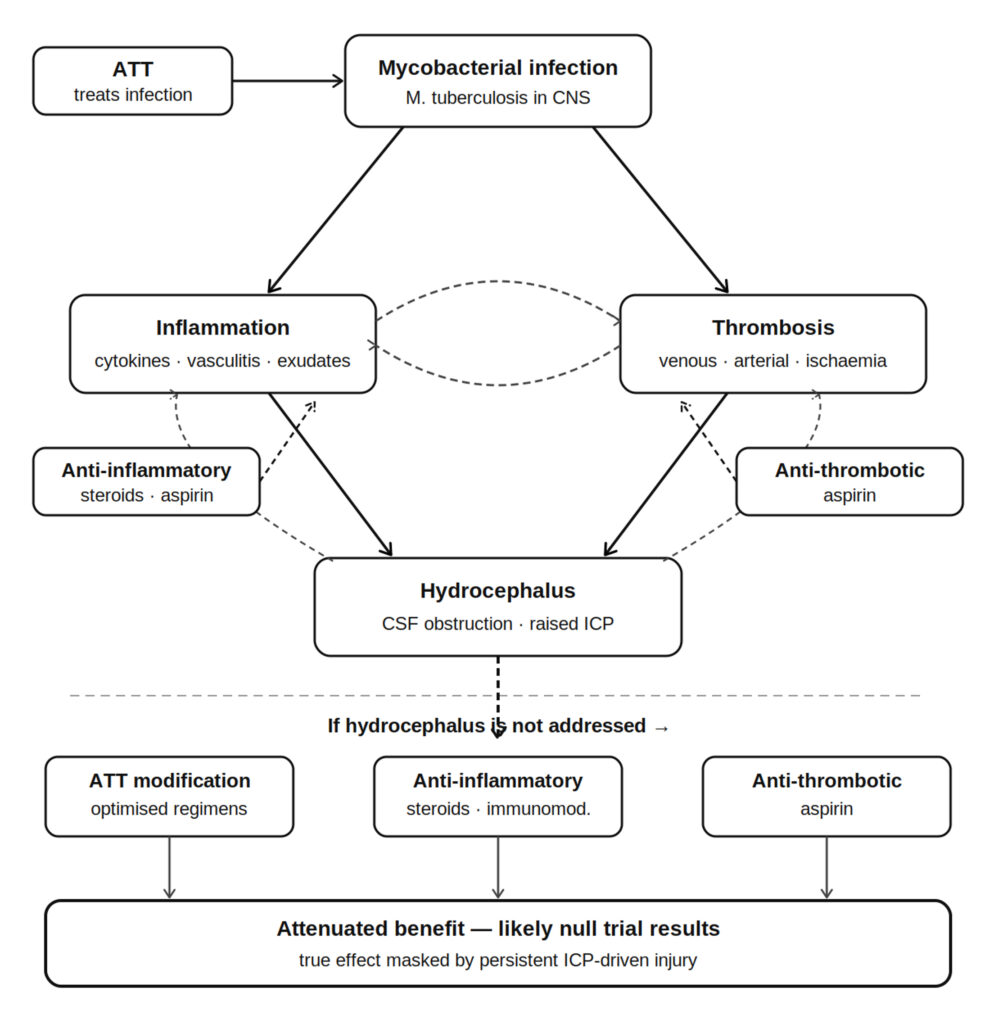
This possibility introduces a competing-risk framework that has received relatively little attention in TBM trials. Mortality may arise through at least two overlapping pathways: an early pathway related to intracranial hypertension and secondary brain injury, and a later pathway related to persistent infection, inflammation, or their complications. Existing therapeutic trials are largely designed to influence the latter while providing limited standardization of the former. As a result, variability in the detection and management of hydrocephalus, particularly the timing and availability of cerebrospinal fluid (CSF) diversion procedures, may introduce unmeasured confounding and complicate interpretation of observed treatment effects7.
At the same time, caution is warranted when interpreting the relationship between hydrocephalus and outcome. Hydrocephalus should not automatically be viewed as a causal explanation for poor prognosis. Although numerous studies4-6 have demonstrated an association between hydrocephalus and mortality, association alone does not establish causality. Similarly, the effectiveness of CSF diversion is likely influenced by several factors, including timing of intervention, patient selection, neurosurgical expertise, imaging availability, and healthcare infrastructure. These factors vary substantially across TBM-endemic settings and may themselves influence outcomes.
Nevertheless, the persistently high mortality observed across modern TBM trials raises the possibility that inadequate control of intracranial physiology may contribute to adverse outcomes. In settings where neurosurgical intervention is delayed or reserved for advanced clinical deterioration, patients may progress beyond the threshold of reversible injury. Under such conditions, even highly effective antimicrobial regimens may demonstrate only modest benefits because an important component of mortality lies outside their primary mechanism of action.
The implications for trial design are considerable. Hydrocephalus is commonly treated as a baseline characteristic when it is considered at all. In reality, it is a dynamic process whose severity may evolve over time and whose management varies during the course of illness. Failure to account for these temporal relationships may introduce time-dependent confounding and limit causal interpretation of trial results.
Future TBM studies should therefore incorporate intracranial pathophysiology more explicitly into both design and analysis. Potential approaches include standardized radiological grading of hydrocephalus, serial assessment of intracranial physiology, prospective documentation of the timing and modality of CSF diversion procedures, and pre-specified analyses according to hydrocephalus severity. From an analytical perspective, incorporation of hydrocephalus and CSF diversion as time-updated variables, together with competing-risk approaches and sensitivity analyses addressing differences in neurosurgical access, may improve estimation of treatment effects. More broadly, studies should consider protocolized strategies for the early recognition and management of intracranial hypertension rather than treating it as an external and uncontrolled variable.
Reframing TBM in this manner moves the field beyond a narrow focus on antimicrobial optimization toward a more integrated understanding of disease pathophysiology. Outcomes are determined not solely by eradication of Mycobacterium tuberculosis, but by the interplay between infection, inflammation, vascular injury, and intracranial dynamics. Until these processes are more comprehensively measured and incorporated into clinical trials, the effects of therapeutic interventions may be more difficult to estimate accurately.
We emphasize that this framework should be viewed as a hypothesis-generating perspective rather than a definitive explanation for previous neutral trial results. Future prospective studies incorporating detailed assessment of hydrocephalus, intracranial pressure, and CSF diversion practices are required to determine the extent to which intracranial physiology influences observed treatment effects and clinical outcomes in TBM.
Conflicts of Interest:
The authors declare no conflicts of interest.
Funding:
None.
Ethics Approval and Informed Consent:
Not applicable. This manuscript is an editorial article and does not involve human participants, patient data, animal experiments, or identifiable personal information.
Authors’ Contributions:
PKT conceived the manuscript, developed the conceptual framework, drafted the manuscript, and revised the final version. NG critically reviewed the manuscript and contributed to the interpretation of the concepts presented. All authors read and approved the final manuscript
ORCID ID:
Praveen Tirlangi: 0000-0002-5926-5885
AI Disclosure:
ChatGPT (OpenAI) was utilized solely for language editing and grammatical refinement. All scientific content, interpretations, and conclusions were independently verified by the authors, who take full responsibility for the integrity of the work.
References
- Donovan J, Bang ND, Imran D, Nghia HDT, Burhan E, Huong DTT, Hiep NTT, Ngoc LHB, Thanh DV, Thanh NT, Wardhani ALS, Maharani K, Gasmara CP, Hanh NHH, Oanh PKN, Estiasari R, Thu DDA, Kusumaningrum A, Dung LT, Giang DC, Ha DTM, Lan NH, Chau NVV, Nguyet NTM, Geskus RB, Thuong NTT, Kestelyn E, Hamers RL, Phu NH, Thwaites GE. Adjunctive dexamethasone for tuberculous meningitis in HIV-positive adults. N Engl J Med 2023; 389: 1357-1367.
- Donovan J, Duc Bang N, Dong HKT, Ho DTN, Nguyen TAT, Nguyen TTH, Lam HBN, Phung VKN, Nguyen TT, Nguyen HHH, Pham KNO, Do DAT, Nguyen TMT, Dang TMH, Nguyen HL, Nguyen VVC, Hoang TH, Tran DD, Phung KL, Ramakrishnan L, Le THN, Nguyen TTT, Wolbers M, Kestelyn E, Geskus RB, Nguyen HP, Thwaites GE. Genotype-stratified adjunctive dexamethasone for tuberculous meningitis in HIV-negative adults: a randomized controlled phase 3 trial. Nat Med 2026; 32: 849-858.
- Meya DB, Cresswell FV, Dai B, Engen N, Naidoo K, Ganiem AR, Imran D, Kabahubya M, Lessells RJ, Yunivita V, Estiasari R, Tugume L, Hlabisa B, Kurniawati MY, Sagita N, Kagimu E, Maharani K, Gakuru J, Gaharu MN, Mugabi T, Kimuda S, Namombwe S, Te Brake L, Aarnoutse R, Svensson EM, Bangdiwala AS, Namanda S, Bahr NC, Musubire AK, Moosa MYS, Hamers RL, Marais S, Boulware DR, van Crevel R, Ruslami R. Trial of high-dose oral rifampin in adults with tuberculous meningitis. N Engl J Med 2025; 393: 2434-2446.
- Raut T, Garg RK, Jain A, Verma R, Singh MK, Malhotra HS, Kohli N, Parihar A. Hydrocephalus in tuberculous meningitis: incidence, its predictive factors and impact on the prognosis. J Infect 2013; 66: 330-337.
- Yiek SH, Wong AS. Challenges and controversies in the management of tuberculous meningitis with hydrocephalus: a systematic review and Sarawak institution’s experience. Asian J Neurosurg 2022; 17: 189-198.
- Huang HJ, Ren ZZ, Dai YN, Tong YX, Yang DH, Chen MJ, Huang YC, Wang MS, Zhang JJ, Song WY, Pan HY. Old age and hydrocephalus are associated with poor prognosis in patients with tuberculous meningitis: a retrospective study in a Chinese adult population. Medicine (Baltimore) 2017; 96: e7370.
- Hasib SA, Rizvi I, Garg RK, Bajaj A, Malhotra HS, Kumar N, Uniyal R, Pandey S, Verma R, Sharma PK. Prognostic model to predict outcome of adult patients with tuberculous meningitis undergoing ventriculoperitoneal shunt surgery: a prospective observational study. World Neurosurg 2025; 194: 123562.
To cite this article
Hydrocephalus as the missing variable in tuberculous meningitis trials
Infectious Diseases and Tropical Medicine 2026;
12
: e1865
DOI: 10.32113/idtm_202607_1865
Publication History
Submission date: 20 Apr 2026
Revised on: 13 May 2026
Accepted on: 25 Jun 2026
Published online: 03 Jul 2026

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.